Toggle navigation
Menu
Home
About
PROMOTIONS
Services
ADHD Assessment and Management
Exercise Programming and Support
6-Pillar Balance: Chronic Disease Prevention | Reversal
Dietetics
Peri menopause/ Menopause Management & Support
BLOG
Pricing
Contact
BOOK NOW
Blog
Educational resources for our patients.
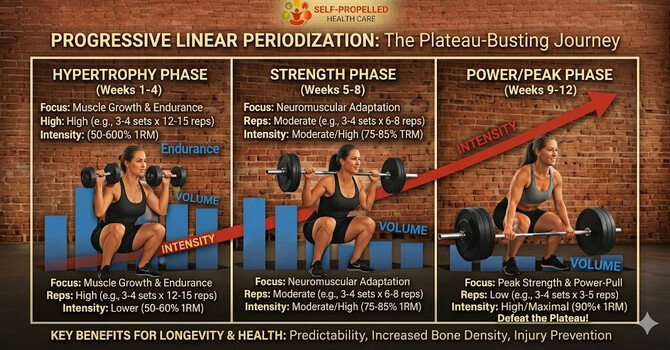
Progressive Strength Training
Defeating the Dreaded "Plateau"
C. Remi
April 27, 2026
The Menopause Transition
The Menopause Transition: What the Science Actually Says about HRT We've all heard the buzzwords-"bio-identical,"...
C. Remi
April 15, 2026
The Women's Health Initiative
Out with the old, in with the new
February 11, 2026
×